Introduction
Humans exist as men and women. Sexual dimorphism predominates in most recent species on the evolutionary scale, including most animals and some plants1. Why is it so? Sex complementarity confers reproductive advantage at the population level, allowing the admixture of distinct genetic traits that would favor adaptation to changing environments through natural selection1,2. In addition, sexuality in humans is crucial for establishing unique social relationships, and conjugal love is its maximal expression. Both unitive and procreative purposes of sexuality in humans uniquely contribute to individual flourishing3,4.
The distinction between sex and sexuality derives from considering biology and psychological/sociocultural factors as major determinants, respectively. Binarism is clear for sex (male or female), which is based on an XX or XY chromosome load. The differential biology of human cells in men and women can be observed in various aspects, including metabolism and disease risk5. Biological anomalies in sex determination may occur and are acknowledged as disorders of sex development (DSD), formerly intersexual states6. These are rare conditions clinically significant in 1 in 1500-4500 live births7.
Beyond biological sex, the term sexuality refers to a constitutive dimension of the person that includes sexual orientation/attraction and self-identity. The spectrum of sexuality is wider than dimorphic biological sex and could somewhat be considered bimodal (Fig. 1). Masculinity and femininity can be graded. Besides genetic determinants, sociocultural factors modulate sex drive and gender identity8. The extent of attraction for the opposite sex and self-recognition as male or female varies from one person to another. However, in a subset of individuals, feelings are not aligned with the biological sex. These atypical behaviors are acknowledged as homosexuality and gender dysphoria, respectively9.
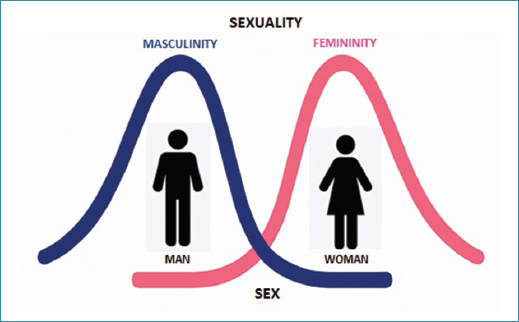
Figure 1. Sex is binary and sexuality is bimodal.
Globally, around 7-8% of the population displays sexual behaviors that do not fit well within the classical male or female sexual orientation and/or self-identity10. Large differences exist between geographical regions and groups belonging to distinct religions and cultures11. Age is a major determinant of atypical sexuality in Western societies. In the UK, the proportion of individuals acknowledging having had same-sex intercourse rose 4-fold from 1940 to 1970 in both men and women (Fig. 2)12.
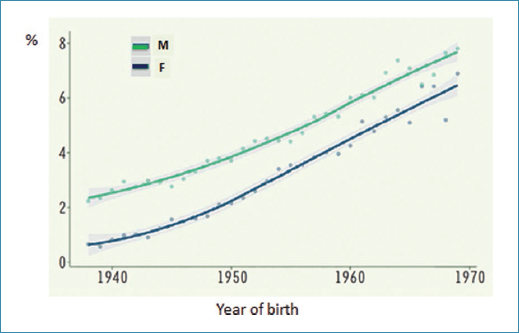
Figure 2. Proportion of adults in the UK BioBank acknowledging having had same-sex intercourse.
In the United States, with 1 in 10 millennials and 1 in 5 Generation Z members identifying as LGBT, this group will exceed 10% of the general population within a couple of years (Fig. 3)13.
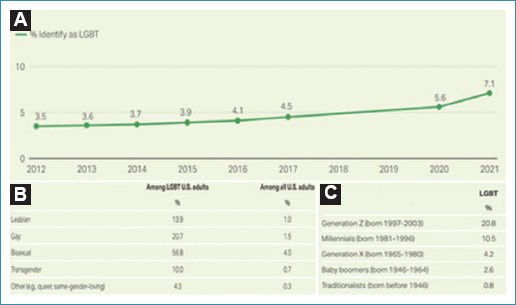
Figure 3. Interviews in 12,000 adults in the United States (2022)13. A: time trends, B: rate and distribution, C: by generation.
The International Classification of Diseases, Eleventh Edition, considers many of the atypical sexual behaviors within a category of compulsive disorders along with hypersexuality that may interfere with regular, ordinary life, job performance, and social relationships14. On the other hand, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition includes sexual dysfunctions, gender dysphoria, and paraphilias within the list of mental disorders15.
Normal sexual development
Sexual phenotype and behavior result from the functional expression of different genes that play roles in sex determination, differentiation, and attitudes from the embryo stage to adult life16. In humans, the default sex development pathway is female. The presence of an intact Y chromosome is essential for male development17. At 6 weeks of life, both the Müllerian and Wolffian duct systems are present, and the embryonic gonads, consisting of the cortex and medulla, are still undifferentiated. From week 6 onward, the testis-determining factor encoded by the SRY gene on the Y chromosome initiates a sequence of events that prompts the gonads to develop into testes. By week 9, Leydig cells appear and start releasing testosterone. There is stimulation of the Wolffian ducts, which ultimately leads to the differentiation of the male genital tract. In parallel, the Sertoli cells produce anti-Müllerian hormone, causing the regression of the Müller ducts and female gonads.
All tissues of the male embryo and fetus have been exposed to testosterone since the 2nd month of life. Testosterone produced by the developing testis can enter the brain. Within certain encephalic regions, testosterone is converted into estradiol, a potent estrogen, by the enzyme aromatase. Estrogens act on estrogen receptors in the brain, influencing the organization and differentiation of neural circuits, also known as the connectome18 (Fig. 4). This process is crucial for sexual differentiation of the brain, affecting neuroanatomy and sexual orientation and identity later in life19–21. This aromatization explains how testosterone influences typical male brain development indirectly through estrogen receptors. In female fetuses, the presence of alpha-fetoprotein binds to circulating maternal estrogens, preventing them from crossing the blood-brain barrier and thereby preventing masculinization of the female brain22.
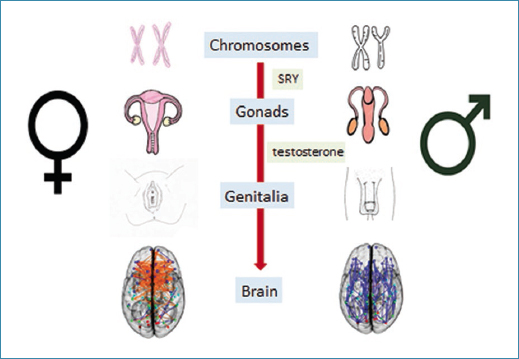
Figure 4. Biological determinants of human sex.
The development of sexually dimorphic brain regions occurs under the direct influence of androgens before and after birth23,24. Early testosterone exposure influences childhood gender role behavior, including sex-typical toy play, as well as gender identity and sexual orientation25,26. The sexually dimorphic nucleus of the preoptic area (SDN-POA) is the earliest sex difference reported in the mammalian brain27. This small collection of neurons is larger in males than in females. A smaller SDN-POA correlates with a preference for mating with males. In experimental studies, increasing the number of neurons in the SDN-POA in neonatal females resulted in the loss of preference for male odors in adulthood, an effect paralleled by dampened excitation of SDN-POA neurons27.
Besides playing an essential role in the sexual differentiation of brain and behavior, gonadal hormones in adulthood shape sexually dimorphic neural circuits28. Sex hormones activate these neural networks, promoting the expression of sex behavior, including its two categories, appetitive and consummatory29.
A large neuroimaging study examined 949 youth aged 8-22 years from diverse ethnic backgrounds30. Male brains had more white matter, whereas female brains had more gray matter. Males had more intrahemispheric connections, whereas females had more interhemispheric connections. Neuroanatomical regions were more active for motor movements and coordination, spatial skills, and physical aggression in males. In contrast, brain areas more active in females were involved in language and communication skills, memory, and intuitive analyses30.
It is interesting to note that all estrogens are synthesized from androgens. Both ovaries and testes can produce these. The amount of androgens produced and the proportion converted to estrogens significantly differ between males and females. Systemic levels of estrogens are largely determined by the activity of the aromatase enzyme (cytochrome P-450 19), which is primarily present in the liver and adipose tissue. At puberty, phenotypic effects of testosterone include secondary male sex characteristics and sex drive. Estrogens produce breast development and menstrual flow in females. Recent evidence also suggests that perinatal ovarian hormones influence sexual orientation and attraction for men31. However, unlike testosterone in men, estrogens are not responsible for female sexual excitement or sexual satisfaction, which may be partly due to testosterone5.
Disorders of sex development
Around 1-2% of the population suffers from congenital disorders involving atypical development of chromosomal, gonadal, or anatomical sex32,33. These conditions were formerly known as intersexual states or “pseudohermaphroditism”34,35. The 2005 Chicago Consensus Meeting marked a turning point, deeming these terms outdated6. Instead, the category DSD was introduced along with a more systematic classification and nomenclature, categorizing DSD into three main groups: (i) chromosomal DSD, (ii) 46 XX DSD, and (iii) 46 XY DSD. In the absence of genotypic characterization, reporting individuals presenting with ambiguous genitalia could be more clinically helpful35.
Among the most frequent sex chromosomal DSDs are aneuploidies, such as Klinefelter syndrome (47 XXY) and Turner syndrome (45 XO). Overall, sex chromosome trisomies remain largely underdiagnosed33. For 46 XX DSD, the most common are females with congenital adrenal hyperplasia or the Mayer-Rokitansky-Küster-Hauser syndrome32. For 46 XY DSD, the most frequent conditions are androgen insensitivity syndromes32 (Table 1). Clinical manifestations of DSD can be recognized at birth or may appear at the pubertal age or later in adulthood as infertility.
Table 1. Classification and major disorders of sex development
| Group | Prevalence among newborns (per 100,000) |
|---|---|
| Sex chromosomal DSD | |
| 45 XO (Turner syndrome) | 25-85 |
| 47 XXY (Klinefelter syndrome) | 60-150 |
| 46 XX DSD | |
| Congenital adrenal hyperplasia | 3-6 |
| Uterine atresia and vaginal hypoplasia (Mayer-Rokitansky-Küster-Hauser syndrome) | 10-20 |
| 46 XY DSD | |
| Androgen insensitivity syndromes | 4-6 |
|
DSD: disorders of sex development. |
|
The management of DSD has classically involved pediatric services of endocrinology and surgery. Awareness of the need to involve multidisciplinary teams and long-term caring, including transfer to adulthood, has steadily occurred. Urologists, psychiatrists, and psychologists are nowadays part of many DSD care teams. Many DSD persons will be infertile, but other aspects of sexual life and cancer risk should be addressed36,37.
Same-sex attraction
It is important to differentiate sexual conditions of biological basis from disorders of the sexual sphere, such as same-sex orientation and transgender identity, that largely result from acquired determinants (social, cultural, etc.)38 (Table 2). Accordingly, whereas heritability is above 80% for height, type 1 diabetes, or schizophrenia, it stays below 40% for homosexuality12.
Table 2. Major disorders of the sexual sphere
| Intersex states (differences of sex development) |
| Same-sex attraction |
| Transgender identity |
| Hypersexuality – sexual promiscuity, sex addiction |
| Paraphilias: exhibitionism, voyeurism, fetishism, sadism, masochism, pedophilia |
Despite having a phenotypic male or female appearance, some individuals manifest sexual attraction to persons of the same sex. Sexual feelings during adolescence are frequently unstable, and affections and sex drive may be confounded. Having the opportunity to chat with parents, close relatives, teachers, and/or tutors about the meaning of sex and sexuality may help to mature sexual behavior. Failure to know the purpose of sex may result in gaps in personality building. However, same-sex orientation is a disposition distinct from manifestations and behaviors, as previously acknowledged, distinguishing appetite and consummation29. In fact, it could never be manifested39. However, any sexual activity is rewarding and reinforcing, and same-sex orientation can be fed with behaviors28.
The prevalence of same-sex orientation varies across regions, cultures, sexes, and age ranges. In Western countries, it can be recognized by roughly 7-8% of the population40. In a representative sample of 5000 youth in Spain interviewed in the year 2020, the proportion acknowledging homosexuality was 8%, greater in boys than girls (10% vs. 6.1%, respectively) (Fig. 5). Of note, bisexuality was overall reported by 8.6% of youth, being more frequent in women than men (12% vs. 5%, respectively)41.
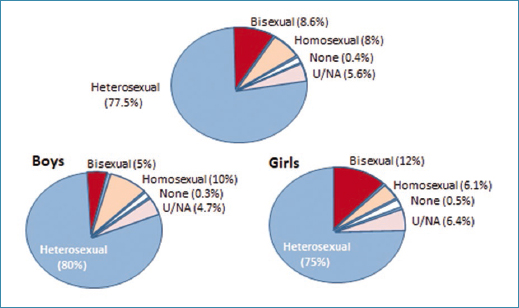
Figure 5. Interviews on sexual orientation in 5,000 youth in Spain (2020)41.
Thanks to twin studies, it has been known for decades that human same-sex attraction has some heritable component42. The largest study on same-sex orientation in twins was conducted in Sweden and included 7652 same-sex pair individuals43. Overall, same-sex behavior was relatively rare (4%). It was more frequent in females and monozygotic twins. In men, heritability accounted for 39%, and unique environmental factors accounted for 61% of same-sex behavior. In women, genetics explained 18% and sociocultural variables explained up to 66%. A shared environment explained 16%. This weaker heritability effect in women has been highlighted in other studies. Among the unique environmental factors, prenatal exposure to sex hormones appears to play the most significant role25.
One study of practically the whole Swedish-born population over the age of 25 reported an elevated risk of depression, substance abuse, and attempted or completed suicide in same-sex (compared to opposite-sex) married individuals44. This elevated psychiatric risk persisted when same-sex married individuals were compared with their opposite-sex married siblings, which is consistent with a substantial role of familial common causes (e.g., genetic and shared environmental)45,46.
In the largest genomic study conducted so far, nearly half a million persons were asked to self-report same-sex behavior. No gay gene was found47. Instead, many polymorphisms were found to influence same-sex orientation, each with a tiny weight. This lack of biological determinism for same-sex points out the importance of social and cultural factors12. In other words, the distinction between “nature” and “nurture” should prevail when considering disorders of the sexual sphere (Fig. 6). At the same time, it is worth acknowledging that men and women are not just born but only grow. They are both born and grow.
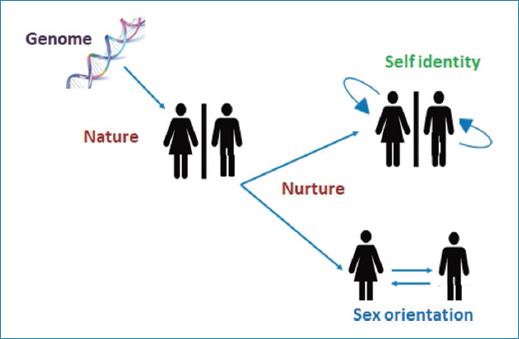
Figure 6. Biological and sociocultural determinants of sexuality. “Nature” versus “Nurture.”
Last century, Simone de Beauvoir claimed that “woman is not born but rather becomes,” meaning that femininity is not innate but a social construct48. Accordingly, each person should make the choice for sex preferences and identity, disregarding the biology and the sociocultural environment. In contrast, Brendan Zietsch, the leading researcher of the UK Biobank and 23andMe large genome study reported above47 defends that his study demonstrated a limited but clear role of genes in determining same-sex behavior49. However, altogether genetic variants accounted for just 8-25%, and no single variant accounted for more than 1%. Thus, same-sex behavior is a strongly polygenic trait, and environmental determinants, including prenatal factors and sociocultural influences, play a more important role50.
Why has same-sex behavior in humans been maintained despite the fact that it apparently does not offer any evolutionary advantage? No doubt, it is somewhat of an evolutionary paradox. The explanation for the persistence of genetic variants associated with same-sex behavior, despite their apparent fitness costs, remains uncertain. Zietsch’s team has proposed that genetic variants associated with having more sex partners could provide a mating advantage among heterosexuals51 and, in this way, favor the persistence of such variants at the population level.
Zietsch has finally claimed that his research should inform sexology more widely. The traditional and most popular measure of sexual orientation is the Kinsey scale52, which is bipolar and implies a continuum between “exclusive heterosexuality” and “exclusive homosexuality. It inappropriately measures homosexuality and heterosexuality on a single-dimensional scale, making one trade-off for the other53. However, individuals can be high on both same-sex and opposite-sex behavior or attraction (some bisexual individuals), and others can be low on both (asexual). Thus, Zietsch considers that there is no continuum from exclusively opposite-sex to exclusively same-sex behavior. Therefore, the Kinsey scale should be abandoned53.
Gender dysphoria
Some individuals acknowledge discomfort between their biological sex and their feelings and wishes. They desire to be of the opposite sex. This discordance between body appearance and psychological, sexual identity is known as gender dysphoria. Historically, there have been individuals who, from an early age, exhibit behaviors typically associated with the opposite sex. Boys acting with feminine traits and girls with masculine behaviors have always existed. However, news on transgender people has risen in an unprecedented way during the last two decades54,55.
Three differences between the surveyed data and media representations stand out: (1) while the media focus on male-to-female individuals, most transgender people in Western societies today are female-to-male; (2) Western media representations of transgender individuals often highlight glamorous and successful individuals. However, empirical data show that the socioeconomic status of transgender individuals tends to be lower than that of non-transgender people; and (3) the transitioning process of transgender people is often portrayed as a successful soteriological journey of becoming one’s “true self.” However, medical surveys show that transgender people frequently suffer from psychological and physical problems both before and after transitioning. Altogether, the disparity between the empirical data and the media narratives on transgender people is due to the persistence of neoliberal narratives in Western media56.
Sexologist Michael Bailey, from Northwestern University in Chicago, has analyzed 1655 American adolescents with rapid-onset gender dysphoria, which many consider to be the result of social contagion and not a true medical condition57. In 75% of the cases, they were girls between 11 and 21 years old. Of note, the frequency of mental disorders (anxiety, depression, and attention deficit hyperactivity syndrome) was more frequent in this group. Many of the parents said they felt pressured by health care staff who cared for their daughters and took care of the sexual transition with hormone therapy and corrective surgery. Those same parents noted that the mental health of many of their daughters worsened after transitioning.
Gender ideology defends that sex-discordant gender identity is the result of a bodily defect present within an individual with normal psychological function. Thus, it is hypothesized that health will be restored if the body is changed to align with gender identity. Conversely, the premise that sex-discordant gender identity is largely influenced by, or the result of, psychological factors leads to defending that health will be restored by addressing the contributing psychological difficulties58.
Interventions with pubertal blockers, such as GnRH agonists and/or cross-sex hormones, have not demonstrated benefits in treating gender dysphoria58,59. On the contrary, they may produce metabolic, cardiovascular, and bone damage60. Despite being a pioneer in supporting sexual transition in youth with gender dysphoria, last year, the UK health system reversed its laws. It suspended the prescription of puberty blockers in minors with gender dysphoria. The UK report notes that these drugs can only be used for research purposes. Furthermore, results from corrective surgery are far from satisfactory36,37,61. The UK decision was significant because it was one of the pioneering countries to approve puberty blockers. Other countries have followed suit and modified their laws.
The complaints of some patients and/or their families have forced the reconsideration of the management of sexual identity problems in the youngest. The closure of the Tavistock Clinic in London in 2022 is a clear example. The cases of repentant trans women have been on the front pages of newspapers, such as that of Keira Bell in England and others62. Experiences of de-transitioners have frequently acknowledged poor baseline psychological assessment63.
Contrary to those who defend hormone therapy for transgender youth, it seems clear that psychological and/or psychiatric assessment is essential in minors who consult for gender dysphoria. The latest has been stated by the European Academy of Pediatrics, which has emphasized the need to assess adolescents globally and address other associated social and mental health disorders that may be present64. Most minors who manifest gender dysphoria may benefit from adequate psychotherapeutic management. Psychotherapy is not conversion therapy, as mistakenly defended by gender-affirming supporters65. With supervised waiting, most youth with gender dysphoria decide not to change their biological sex. This aspect is particularly important in young girls, who are the majority with gender dysphoria, since they will be able to have offspring later on. On the contrary, if the hormone is given early and corrective surgery is performed, the damage could be irreversible59,64,66.
It is important to highlight that the traits of masculinity and femininity in children and adolescents cover a wide spectrum of manifestations. We already discussed that whereas sex is binary, sexuality should be considered as bimodal. Not all boys enjoy aerobic sports competitions, such as soccer or playing with weapons. Similarly, not all girls like playing with dolls, participating in cheerleading, cooking, dressing up, etc. It is important to admit such a wide range of normality without creating doubts about gender identity in youth. Keeping aligned biological sex and sexual identity provides the most natural way to build a healthy personality easily and, in this way, facilitates flourishing2–4.
Concluding remarks
The term “differences” instead of “disorders” of the sexual sphere has been recently proposed for addressing anomalies of sex development of biological basis, since it is more neutral and inclusive. It would emphasize diversity rather than illness32,33. The back side of this willingness to avoid any possible stigma or discrimination is that medical research and funding, as well as the development of treatments, are mainly encouraged when conditions are considered pathologies, since only then can interventions aimed at ameliorating or curing such entities be pursued. On the contrary, if such conditions are interpreted as part of the normal spectrum, acceptance would be the most convenient approach, thereby avoiding the need for modifications38.
The dualism we recognize for sex, men and women, does not exist for body and mind/spirit, as the person is a whole, a dynamic-minded body that is both born and growing. Any of us is defined by biology, psychology, and sociocultural influences. Our unique person is reshaped with elections and behavior. Thus, sexuality issues need to be addressed considering the whole person, respecting autonomy and freedom, but giving information and knowledge that could help to overcome any difficulties.
Sex and sexuality are fundamental parts of the person and are required for achieving human wholeness and flourishing2–4. Sexual disorders and behaviors that distort this critical role deserve to be addressed medically, as the main purpose of the physician’s profession is to look for the patient’s good67. We should respect anyone with atypical sexual phenotypes, but helping to ameliorate suffering from these conditions is warranted. In fact, there is a moral imperative to do so67. Otherwise, advances in scientific knowledge would not translate into improvements in human health for this subset of persons.
Understanding in this way the meaning of sex and its binary nature provides an additional benefit, which is the opportunity to bring back individuals who would reconsider their sexual behavior. As Barbara Golder pointed out in a recent editorial, “these persons are called to fulfill God’s will in their lives,” like anyone, and try to overcome “the difficulties they may encounter from their condition”68.
In summary, following the approach taken for intersex states of biological basis that are nowadays referred to as differences of sex development (DSD), we propose that same-sex attraction and transgender identity could be categorized as differences in sexual orientation and self-identity, respectively. Whereas inclusive efforts for persons with atypical sexuality must be encouraged to avoid discrimination, these conditions should not be overlooked medically. Denying their relevance might discourage research that would ultimately benefit these individuals.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of humans and animals. The authors declare that no experiments involving humans or animals were conducted for this research.
Confidentiality, informed consent, and ethical approval. The study does not involve patient personal data nor requires ethical approval. The SAGER guidelines do not apply.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the writing of this manuscript.
